The ED Gauntlet - A ring of sometimes irrelevant fire
Sitting in our station last night, the local cable channel showed a commercial of an unnamed, regional, academic medical center that is known for excellence in many specialties. We'll call it "Big Hospital X". I felt it was a good piece of marketing, liked the imagery, the aerial views of the facility, the smiling faces of the competent within. It was -- good marketing.
In the middle of the night, we responded to a call for a person with chest pain who had consumed an enormous amount of nitroglycerine (NTG) as in more than five times the prescribed dose, and more importantly, without relief. Some of our most basic training informs us that chest pain that does not respond to nitroglycerine is less likely to be angina and more consistent with someone having a heart attack.
Upon arrival we encounter a strong looking, hulk of a man in his early 60's seated at the dining room table. Long story short, he's had heart attacks in the past, has had coronary artery bypass graft (CABG), has several stents in place and is in agonizing pain. Even without a strong confirmation on our 12-lead EKG showing ***ACUTE MI SUSPECTED***, one doesn't have to be a cardiologist to suspect, he's more than likely infarcting (having a heart attack) again.
We packaged him and gave him medications to prevent platelet aggregation (aspirin), tried 1 dose of our own nitroglycerine (not expecting miracles after all the nitro he took) and a couple doses of fentanyl to try to blunt the man's pain. 100 mcg of fentanyl usually does a pretty decent job of blunting your pain (or at least makes you not give a f' that it's there). We had about a half-hour transport time to Big Hospital X, consulted with the ER physician about what we saw and verified if there was anything else they may want to give. The hulking patient with a soldier's tattoo across their muscular arm was unfazed by anything we gave him. He was in agony.
Finally we arrived at Big Hospital X (the one's with good marketing) and faced "the gauntlet" (intake registration and triage nurse). No, they're not a real gauntlet. They do have an important function to register and screen patients according to severity, available resources and other factors. Sometimes however, they really appear less like a part of our team and more like the healthcare equivalent of an offensive line in football; their principal function being -- keep intruders out -- and protect their quarterback (the docs).
First stop was the registration person. Usually, with acute patients, we bypass the gauntlet and head right back to the resus (resuscitation) room. A registration person will follow us and do a "quick reg" on the fly. Our patient was acutely ill by my assessment, but lacking the horrible ECG finding mentioned above, I suppose, didn't quite fit into their little box as "critical."
After dealing with that slow process came the triage nurse. She didn't seem to be grasping that we likely have a candidate here who is evolving before our eyes into a "STEMI" patient (the most critical type of heart attack). She asked her battery of questions as the man writhed and struggled to contain his pain on our stretcher. Then she comes over and asks "what are his vitals?" and "let me see the 12-lead." This is where this began to approach surrealism. Generally, nurses lack the training to accurately read EKG's other than the obvious label across the top. Second, we have already:
Armed with only a partial story, she then vanishes into another area of the ER to relay her findings to the ER physician and decide whether this patient needs the resus room (most critical area) or a regular ER bed. This was the entire reason WE already consulted with the ER physician. Meanwhile, precious time and quite possibly heart muscle erodes away as we deal with fifty questions.
We're standing in the ER for easily over 10 minutes now or about 9 minutes longer than we should have been there. She re-emerges and begins asking more questions. "Did you call the doctor?"
Lady, we're fucking paramedics. Yes we called the doctor; move! (inside voice)
"Yes ma'am we did." (actual voice)
"Did the nitroglycerine burn?" she asked. My head almost exploded right there.
Are you kidding me? That's a novice's question aimed at ruling out suspicion that the patient's nitroglycerine may have been expired, an old prescription, or exposed to sunlight to degrade its potency. What do the journals say about this? JAMA 1972 Dr. Copelan on the topic; taste "had no value as an index of freshness."1 We already confirmed and reported (to the doctor on the phone and now the gauntlet nurse at the desk) that this is a brand new prescription for NTG that was picked up at his pharmacy today!
For God's sake get out of the way and let us through! (again inside voice).
We finally began walking slowly toward (wait for it...) the resus room. Again, she badgers my partner since, out of frustration, he didn't adequately answer her the first time: "Did the nitroglycerine burn?" Breathless and with an eye-roll, he answered reluctantly; "We didn't ask that" but assured her it's a current prescription.
She pressed my partner as if the presence or absence of a burning sensation from nitroglycerine is of any diagnostic value. It's not. This man needs a cath lab, and if not that, at least needs to not be here in the hallway answering your fifty irrelevant questions!
Before we left, his EKG evolved and they now had their ominous ***ACUTE MI SUSPECTED***
Did I tell you they have great marketing?
References:
In the middle of the night, we responded to a call for a person with chest pain who had consumed an enormous amount of nitroglycerine (NTG) as in more than five times the prescribed dose, and more importantly, without relief. Some of our most basic training informs us that chest pain that does not respond to nitroglycerine is less likely to be angina and more consistent with someone having a heart attack.
Upon arrival we encounter a strong looking, hulk of a man in his early 60's seated at the dining room table. Long story short, he's had heart attacks in the past, has had coronary artery bypass graft (CABG), has several stents in place and is in agonizing pain. Even without a strong confirmation on our 12-lead EKG showing ***ACUTE MI SUSPECTED***, one doesn't have to be a cardiologist to suspect, he's more than likely infarcting (having a heart attack) again.
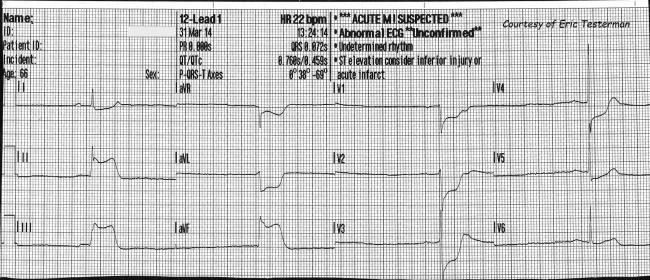 |
| Photo Courtesy - ECG-Guru |
We packaged him and gave him medications to prevent platelet aggregation (aspirin), tried 1 dose of our own nitroglycerine (not expecting miracles after all the nitro he took) and a couple doses of fentanyl to try to blunt the man's pain. 100 mcg of fentanyl usually does a pretty decent job of blunting your pain (or at least makes you not give a f' that it's there). We had about a half-hour transport time to Big Hospital X, consulted with the ER physician about what we saw and verified if there was anything else they may want to give. The hulking patient with a soldier's tattoo across their muscular arm was unfazed by anything we gave him. He was in agony.
Finally we arrived at Big Hospital X (the one's with good marketing) and faced "the gauntlet" (intake registration and triage nurse). No, they're not a real gauntlet. They do have an important function to register and screen patients according to severity, available resources and other factors. Sometimes however, they really appear less like a part of our team and more like the healthcare equivalent of an offensive line in football; their principal function being -- keep intruders out -- and protect their quarterback (the docs).
:format(webp)/cdn.vox-cdn.com/uploads/chorus_image/image/64704773/Screen_Shot_2019_07_10_at_7.50.34_PM.0.png) |
| The Denver Bronco's offensive line |
After dealing with that slow process came the triage nurse. She didn't seem to be grasping that we likely have a candidate here who is evolving before our eyes into a "STEMI" patient (the most critical type of heart attack). She asked her battery of questions as the man writhed and struggled to contain his pain on our stretcher. Then she comes over and asks "what are his vitals?" and "let me see the 12-lead." This is where this began to approach surrealism. Generally, nurses lack the training to accurately read EKG's other than the obvious label across the top. Second, we have already:
- Interpreted the EKG ourselves
- Relayed our findings to the physician and gave the drugs the physician ordered
- Already transmitted a hi-fidelity copy of the EKG to said physician.
Armed with only a partial story, she then vanishes into another area of the ER to relay her findings to the ER physician and decide whether this patient needs the resus room (most critical area) or a regular ER bed. This was the entire reason WE already consulted with the ER physician. Meanwhile, precious time and quite possibly heart muscle erodes away as we deal with fifty questions.
We're standing in the ER for easily over 10 minutes now or about 9 minutes longer than we should have been there. She re-emerges and begins asking more questions. "Did you call the doctor?"
Lady, we're fucking paramedics. Yes we called the doctor; move! (inside voice)
"Yes ma'am we did." (actual voice)
"Did the nitroglycerine burn?" she asked. My head almost exploded right there.
Are you kidding me? That's a novice's question aimed at ruling out suspicion that the patient's nitroglycerine may have been expired, an old prescription, or exposed to sunlight to degrade its potency. What do the journals say about this? JAMA 1972 Dr. Copelan on the topic; taste "had no value as an index of freshness."1 We already confirmed and reported (to the doctor on the phone and now the gauntlet nurse at the desk) that this is a brand new prescription for NTG that was picked up at his pharmacy today!
For God's sake get out of the way and let us through! (again inside voice).
We finally began walking slowly toward (wait for it...) the resus room. Again, she badgers my partner since, out of frustration, he didn't adequately answer her the first time: "Did the nitroglycerine burn?" Breathless and with an eye-roll, he answered reluctantly; "We didn't ask that" but assured her it's a current prescription.
She pressed my partner as if the presence or absence of a burning sensation from nitroglycerine is of any diagnostic value. It's not. This man needs a cath lab, and if not that, at least needs to not be here in the hallway answering your fifty irrelevant questions!
Before we left, his EKG evolved and they now had their ominous ***ACUTE MI SUSPECTED***
Did I tell you they have great marketing?
References:



Comments
Post a Comment